56F Abdominal pain 5 years, ileal perforation 1 year, Lump abdomen 1 month
This is an online e-log book to discuss our patient de-identified health data shared after taking his / her / guardian's signed informed consent. Here we discuss our individual patients' problems through a series of inputs from the available global online community of experts with an aim to solve those patients' clinical problems with collective current best evidence-based information.
This E blog also reflects my patient-centered online learning portfolio and your valuable input in the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and coming up with diagnosis and treatment plans. is an online e-log book to discuss our patient's de-identified health data shared after taking his / her / guardians' signed informed consent. Here we discuss our individual patients' problems through a series of inputs from the available global online community of experts with an aim to solve those patients' clinical problems with collective current best evidence-based information.
A 56 year old female have complaints of pain abdomen since 10 days
History of presenting illness-patient was apparently asymptomatic 6 months ago then she was diagnosed to had intestinal obstruction for which she got operated.Now she has complaints of left iliac fossa pain since 3 months aggregated since 10 days pricking type of pain continuous and associated with fever.
No ho vomiting,diarrhoea
No h/o blood in urine,Malena ,no h/o headacge,dizziness.
No h/o SOB, palpitations,chest pain.
K/c/o intestinal TB 3 years ago(used ATTmedication for 1year)
K/c/o hypothyroidism 10 years ago on thyronorm 50 MCG
K/c/o CAD 6 months aho
N/k/c/o hypertension,diabetes,asthma,epilepsy.
Treatment history
Sx laparotomy for iliac perforation.
Personal history:
Diet :Mixed
Appetite : normal
Sleep: adequate
Bowel and bladder movements: regular
No significant family history
General Examination:
Patient is conscious,coherent and cooperative
Moderately built and nourished
Pallor, icterus, cyanosis , clubbing, Lymphadenopathy -absent
Bilateral pedal edema subsided
Vitals :
PR : 86 bpm
BP : 110/80 mmHg
RR : 16CPM
Temperature : 98.6F
Spo2 : 98 % on RA
GRBS-162 mg/dl
Weight:55kg
SYSTEMATIC EXAMINATION
Abdominal examination
P/A-
Shape.of abdomen-obese
Tenderness- present in left iliac fossa
Palpable mass -No
Hernial.orifices-normal
Free fluid - No
Bruits- No
Liver - Not palpable
Spleen- Not palpable
Bowel.sounds- heard
Cardio vascular system examination
Jvp not raised
Inspection:
Shape of chest - elliptical
No visible pulsations
No engorged veins and scars
Apical impulse not visible
Thrills-no
Cardiac sounds- s1s2 heard
No murmurs
Respiratory Sytem -
Dyspnoea- no
Wheeze- No
Trachea position- central
No adventitious sounds.
CVS
Level of consciousness-consious
Speech- normal
No signs of meningeal irritation.
Motor system:
Rt- UL. LL. Lt- UL. LL
Bulk - normal N. N. N
Tone - N. N. N. N
Power - 5/5. 5/5. 5/5. 5/5
Reflexes:
UL LL
Biceps . 2+. 2+
Triceps. 2+. . 2+
Supinator. 2+. 2+
Knee 2+. 2+
Ankle. 2+. 2+
Sensory system: intact
Co ordination is present
Gait is normal
No Cerebellar signs
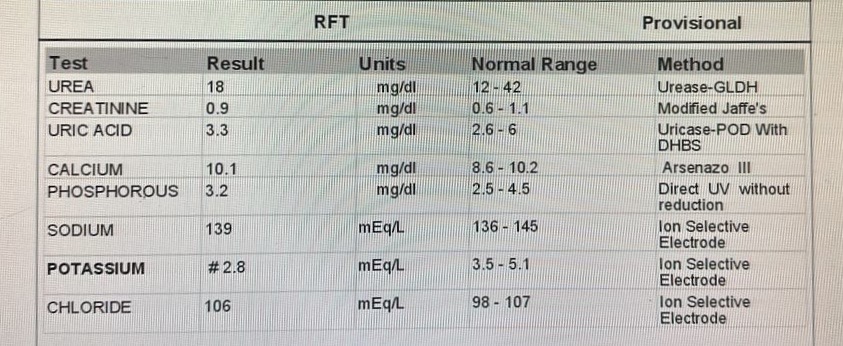
Investigations










Provisional diagnosis
Chrons disease



Comments
Post a Comment